All Pk/Pd models are wrong - but some are more useful.

We have written in previous blogs about the difference between the available models for propofol. Recently, a part of a real clinical case: down-titration using TCI, was shared on LinkedIn, demonstrating some of the consequences of these model differences. We had to make several assumptions regarding the induction phase, but these do not invalidate the simulations.
Case description
A 78-yr-old patient underwent a titrated induction up to an effect-site concentration (Ce) of 1.6 mcg/ml.
Model used: Schnider ( fixed keo), plasma control.
Assumptions: initial concentration 0.8 mcg/, followed by incremental steps of 0.4 mcg/ml when plasma (Cp) and effect-site (Ce) are equilibrated, until final Ce of 1.6 mcg/ml is reached after 25 minutes.
Then, according to the post on linkedIn, burst suppression on the processed EEG (pEEG) is observed, accompanied by loss of alpha activity, necessitating down-titration to 1.1 mcg/ml in 10-min steps. (fig 1)
The final concentration is 1.1 mcg/ml. This case nicely demonstrates the value of processed EEG and the use of TCI.

This raised the question of what concentrations would be calculated using another model that incorporates age directly into its parameters: the Eleveld (+opioid) Model.
Tivatrainer is designed for exactly these type of exercises.
If you have Tivatrainer updated to version 3.0.0 or higher on your smartphone, you can use the Scan QR function available under the 'three-dots' button below any simulation.(see video)
Using the copy-paste function in Tivatrainer, the drug delivery profile from the Schnider simulation in TCI can be applied to the Eleveld (+opioid) model in manual mode so the infusion changes in the Schnider model are recalculated into concentrations in the Eleveld model. (fig 2)
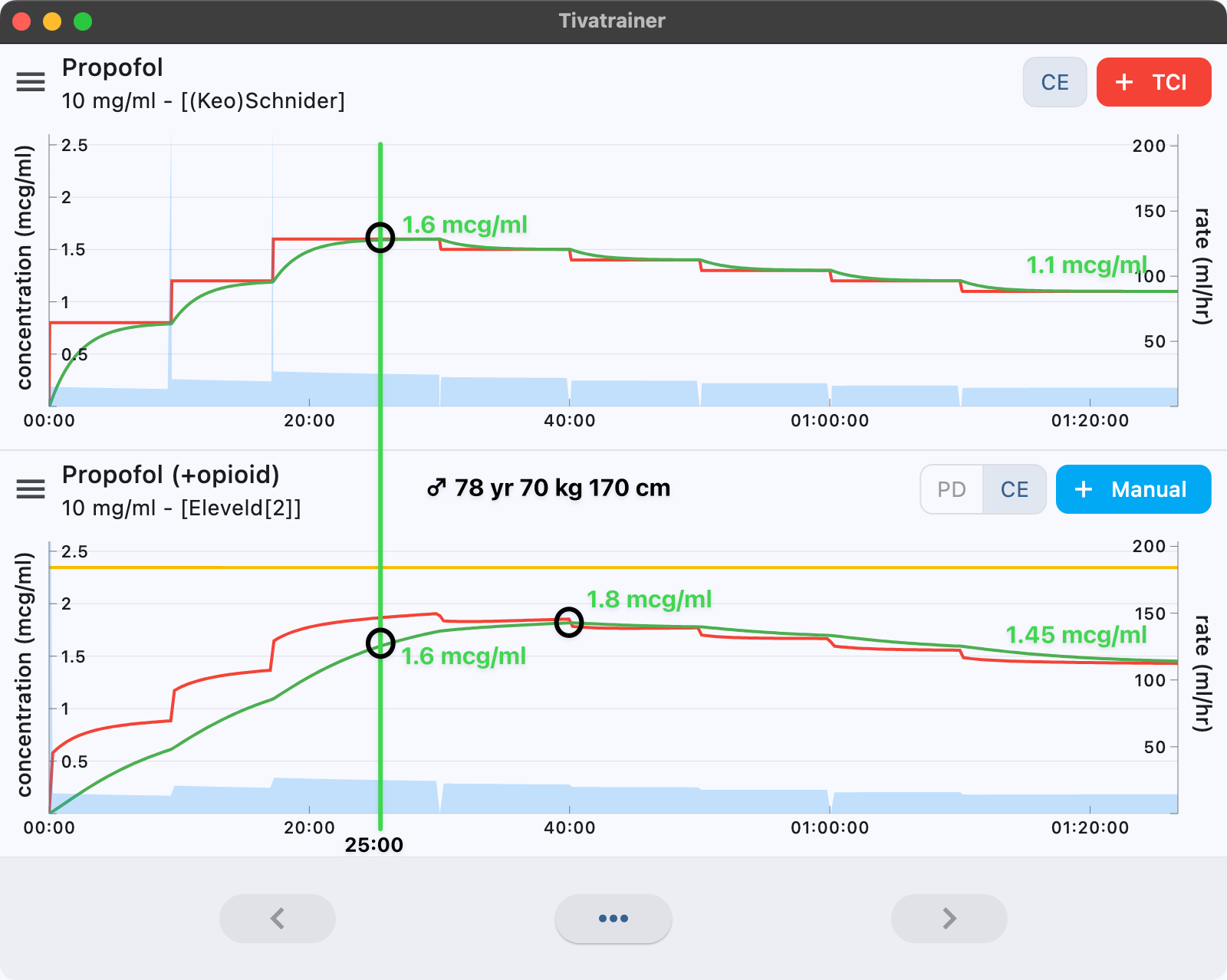
The most prominent difference between the models is the relatively 'slow' and small keo in the Eleveld model, which, even with a slow induction, maintains a concentration gradient between plasma and effect site. However, because of the gradual titration during induction, the difference in Ce at end of induction is only marginal. The Schnider model predicts a Ce of 1.6 mcg/ml after the last equilibration step, which is equal to the prediction in the Eleveld (+opioid) model.
Does this mean there is no clinical difference between the models?
With the Schnider model, a down-titration of 0.5 mcg (from 1.6 to 1.1 mcg/ml) is performed. In the Eleveld model, this same dosing profile corresponds to a decrease of only about 0.15 mcg/ml, resulting in a final Ce of approximately 1.45 mcg/ml. Importantly, the Eleveld model predicts an overshoot to 1.8 mcg/ml. Does this overshoot correspond and explains the observed burst suppression? Hard to say but what we do know is that safety margins in the elderly brain are small. The Eleveld model has a connection between Ce and BIS. You can use the Pharmacodynamic simulation (PD) to show that the BIS at loss of consciousness is predicted to be 64 and then decreasing to 57 when Ce is 1.8 mcg/ml. Because the infusion profile in the Eleveld model is exactly the same as the Schnider model this is also the expected Bis in the Schnider model.
In theory, titration should reduce differences caused by blood-brain equilibration constants between models, leaving only pharmacokinetic differences. However, this is theoretical. In clinical practice, differences between models, including differences in blood effect equilibration, can still influence interpretation and, consequently, control of the patient’s response.
A single example is obviously insufficient to declare one model superior to another. However, the statement of some experts that all models are more or less similar is not supported. Furthermore: the use of a single unified model would represent a major advantage in communication, education and interpretation of TCI behaviour. The adoption of a single model for propofol could also facilitate the future integration of Large Language Models (LLM) into anaesthesia practice.