Remimazolam


Remimazolam: a benzodiazepine like midazolam with engineered pharmacokinetic properties like remifentanil:metabolized by hydrolysis by non specific tissue and plasma esterases. However it seems that a carboxylesterase in the liver is the main responsible for the metabolization. The pharmacokinetics have been described in multiple publication but only recent a population pharmacokinetic model has been published that is suitable to be implemented in a Target controlled infusion system.
Masui, K., Stöhr, T., Pesic, M. & Tonai, T. A population pharmacokinetic model of remimazolam for general anesthesia and consideration of remimazolam dose in clinical practice. J Anesth 36, 493–505 (2022).
Therefore I implemented the model in TivatrainerX and the multiplatform Beta release of Tivatrainer. Below there is a little video that explains the transfer of this model from the internet drug list to the local druglist in TivatrainerX. Verification of that implementation is done with the usual graphical overlaying technique. The author Kenichi Masui has supplied a number of graphs to illustrate the parameterisation of the three compartment model. At the moment the input of the patient parameters in Tivatrainer is fixed so in order to implement the dependency of the clearance on the ASA class I/II or III/IV I have made two selectable versions of the model in the database.
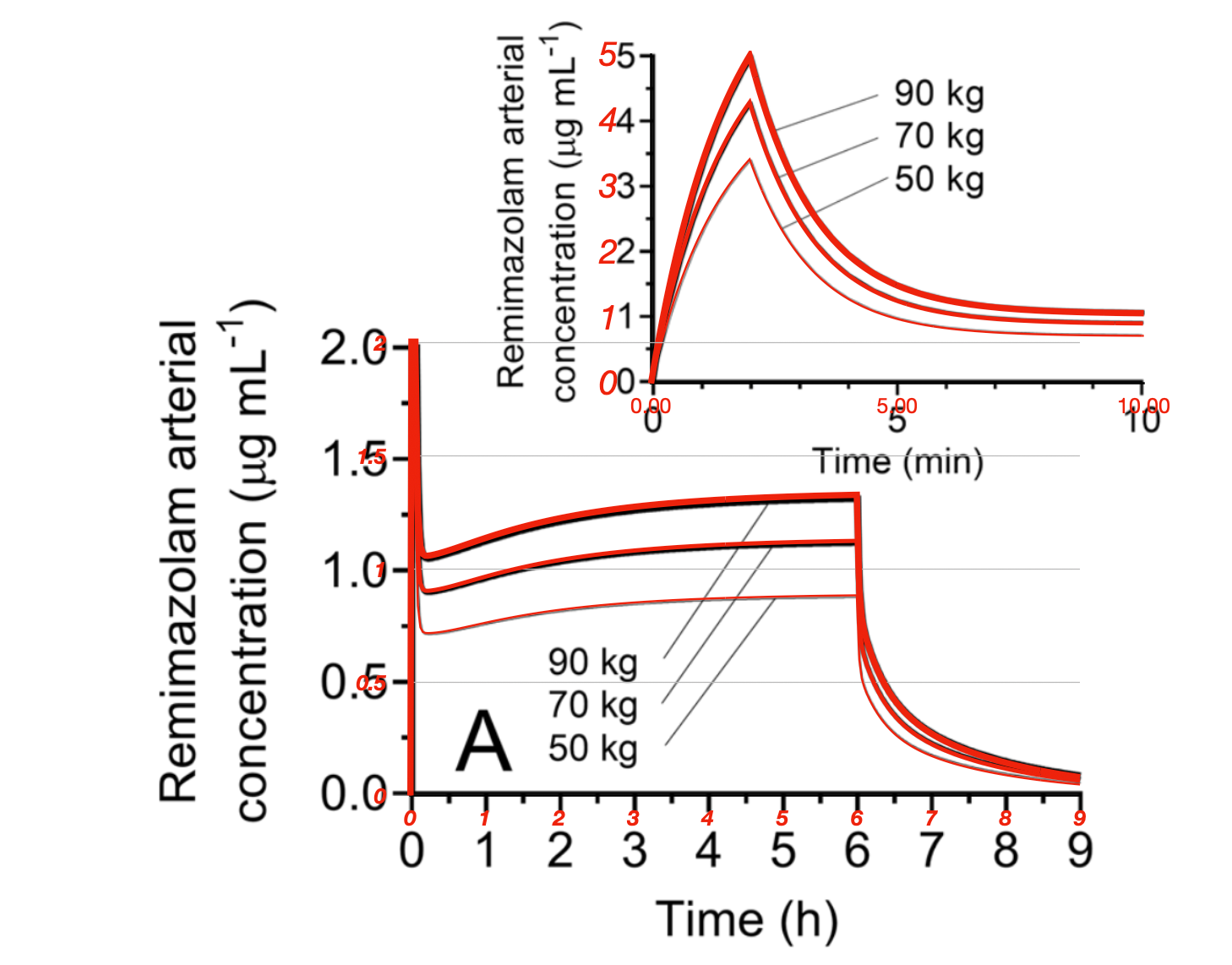
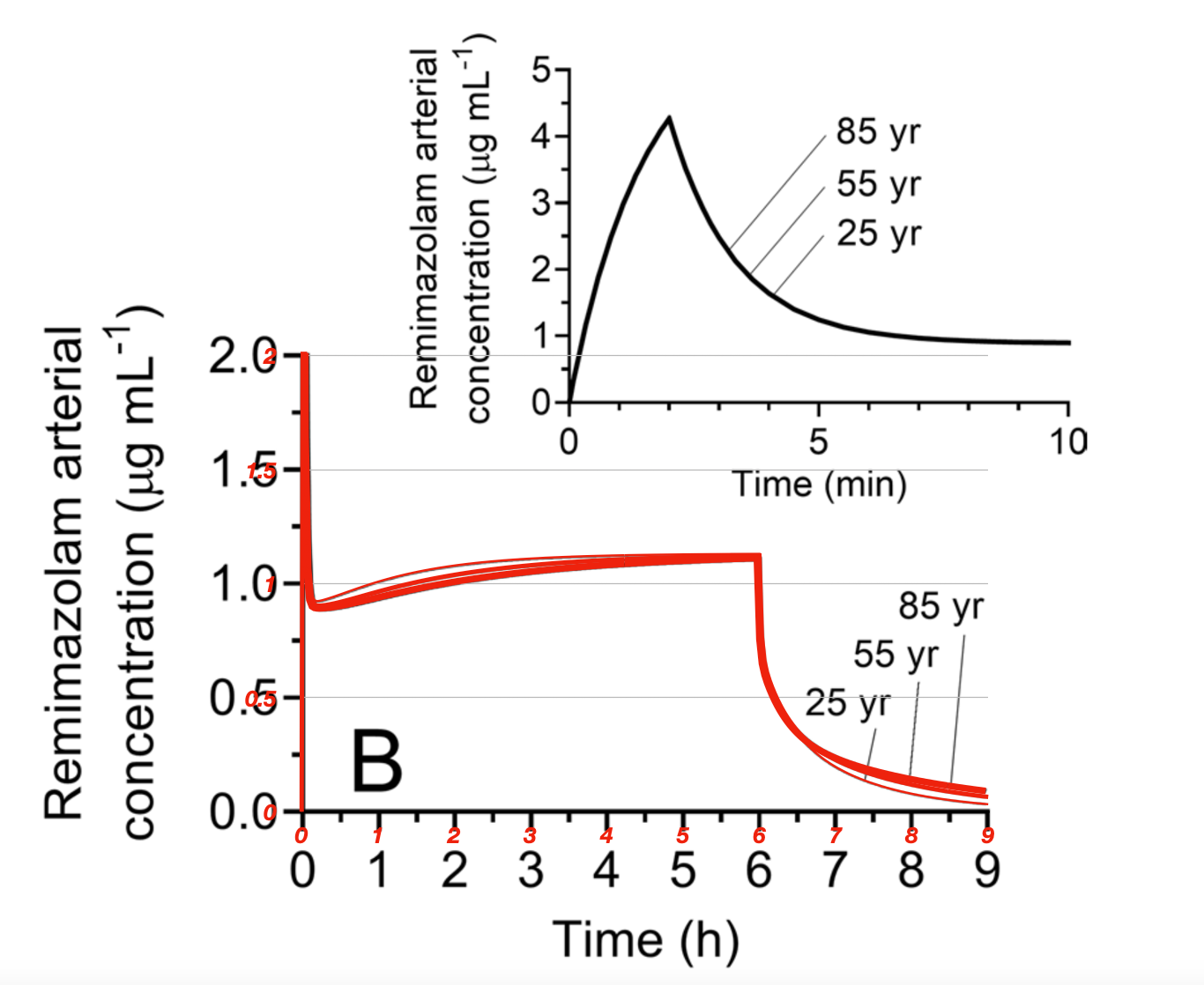
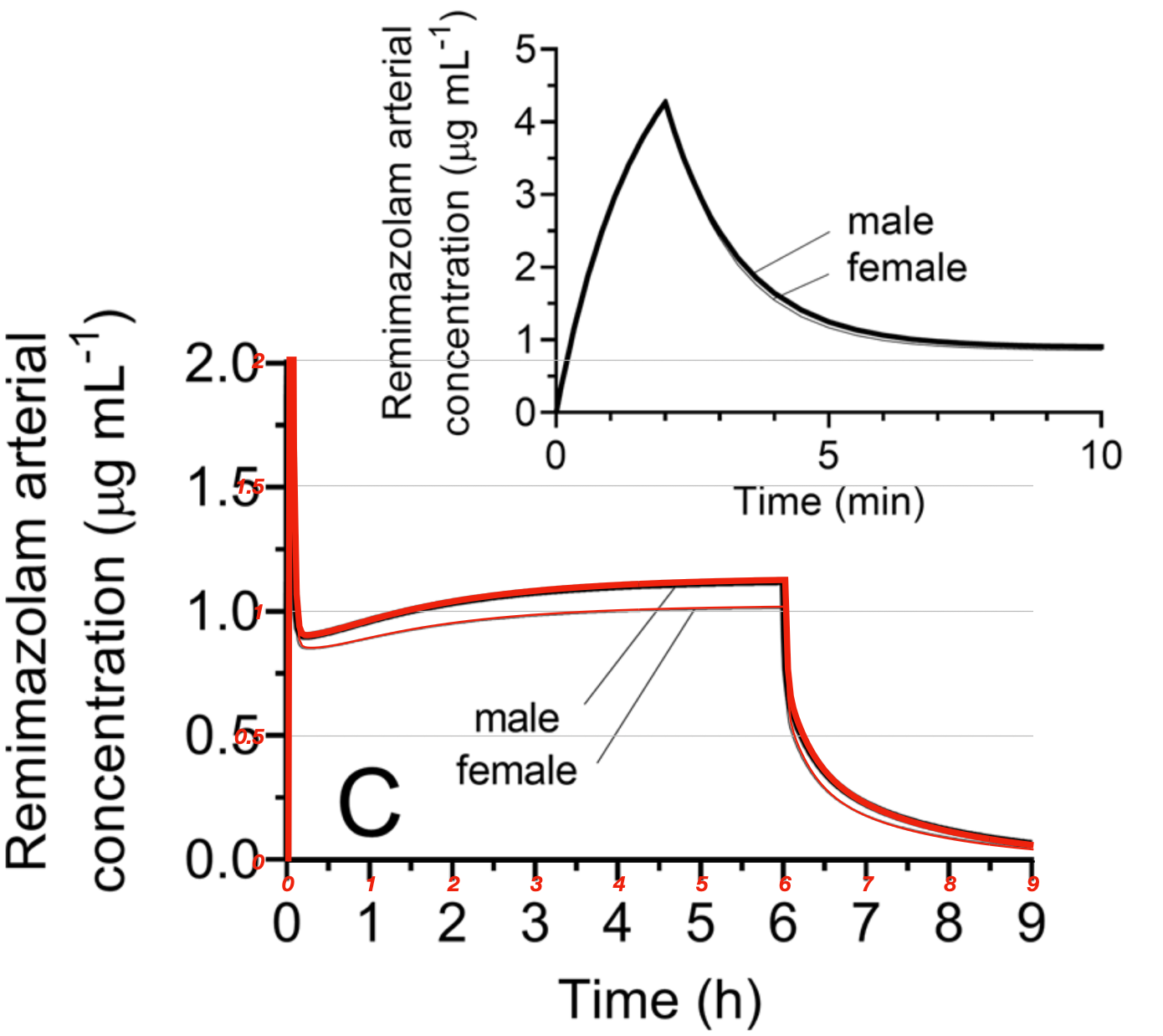
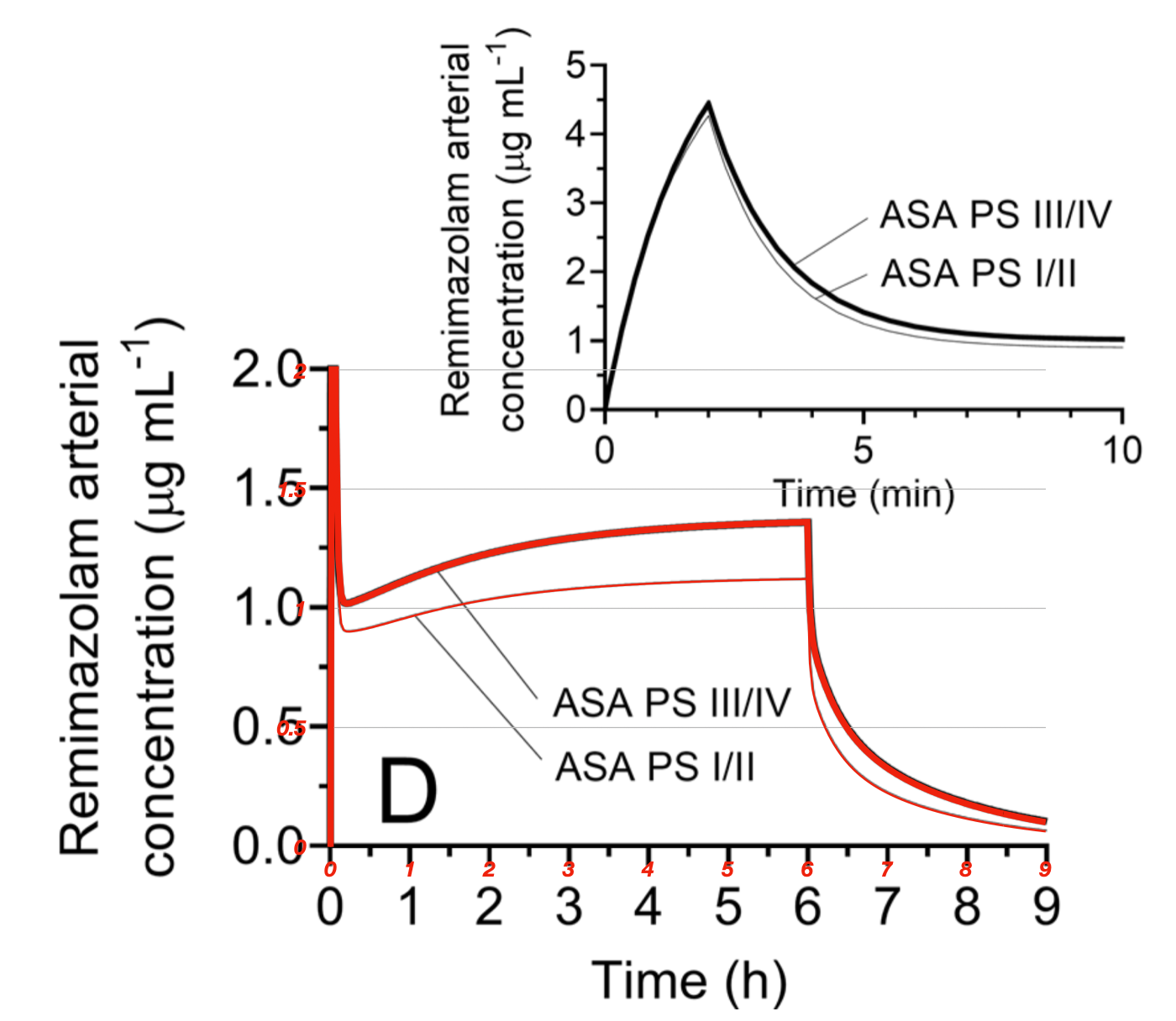
The graphical overlay of the resimulation of Tivatrainer in red over the original pictures in black, show that the implementation is correct and accurate. Only for the weight dependency the early 10 minutes are compared. Doing that for all the graphs would not be more informative than the 6 hr comparison. The dosing was 12 mg/kg/hr the first 2 mimutes and then 1 mg/kg/hr untill 6 hr in a 70kg 170 cm male patient ASAI/II unless specified otherwise. As the dosing was weight based, it is remarkable that the weight(or in fact by the use of the Adjusted Body Weight) still influences the concentration so much. The differences between de weights would obviously disappear if the dose was not per kg Total Body weight but per kg Adjusted Body weight. (nice exercise!). A way to overcome the problems with the parameterisation is to use IVAssist in Tivatrainer that will produce an (adjustable!) infusion scheme for manual dosing as long as no (E)TCI systyem is yet available.
What about the effect site.
The keo for the effect site in this study is derived by Time to peak affect(TPE). This technique is not suitable for specifying a keo for an infusion model like (E)Target Controlled infusion as the TPE is based on a bolus, but this is another discussion. The three compartment model simply cannot handle early-phase pharmacokinetics as it assumes immediate mixing in the central compartment. From propofol we know that the keo tends to be smaller (longer thkeo) when derived from infusion protocols. A smaller(longer) keo will allow a larger loading dose when the model is used in effect site control. The keo derived in this study is already quite small(long) but still, when using effect site control or IVAssist the induction dose is less than used in this study.
For the (still) free beta version of the multi-platform Tivatrainer (https://www.tivatrainer.com) you only need to update the version.
For TivatrainerX some small adaptations in the app are required. The next version(after current version 4.4) that will allow the two remimazolam models(for ASA I/II or ASA III/IV) to be loaded into your TivatrainerX for iPhone/iPad Mac(M1/M2) will be released soon.
In the next blog I will explain how to set up an IVassist simulation, so stay tuned!