Mixing remifentanil in a propofol Target Controlled Infusion device: it is not all white!
Mixing remifentanil in a propofol syringe in a Target controlled infusion device is a practice that is employed specifically for TIVA in paediatric anaesthesia. What are the consequences?


In the previous blogs (https://blog.tivatrainer.com/the-mixifusor-with-tivatrainer-using-the-eleveld-opioid-model/)I have used the copy/paste function of Tivatrainer to analyse a practice that is used by some paediatric anaesthesiologists of mixing remifentanil into one syringe with propofol and put it in a propofol target controlled infusion(TCI) system. This copy/pasting in tivatrainer is very useful, not only for calculating the concentrations when mixing drugs but also to compare the properties of the different pharmacokinetic models or to explain what happens when two syringes are for example accidentally swapped. This copy/pasting follows a couple of rules that are explained here.
| Copy from | Copy to | Content copied |
|---|---|---|
| TCI, ETCI | TCI, ETCI | Targets |
| TCI, ETCI | Manual | Volumes (ml/hr) from source |
| Manual, IVAssist | Manual, IVAssist | Volumes (ml and ml/hr) from source |
| Manual, IVAssist | TCI, ETCI | No copy/paste possible |
Tip: Even without copy pasting you can easily switch in one simulation between TCI and ETCI while maintaining the targets.
Mixing drugs and using TCI is a bad idea for several reasons: mixing can be incompleet, so the concentration in the syringe is possibly not homogenous, there may be juridical consequences in case of a complications and on top of this, the remifentanil concentration becomes unpredictable and dependent on the model that is selected to control the propofol TCI pump.
But admitted: there are also advantages: less equipment and infusion lines and on top: less problems with dead space effects and volume load.
Besides copy/pasting Tivatrainer can also export data to .css files that can be opened by popular spreadsheet programs such as Excel or Numbers. I have used this export function to produce graphs that show the unpredictability of the remifentanil concentration when (E)TCI is used for propofol.
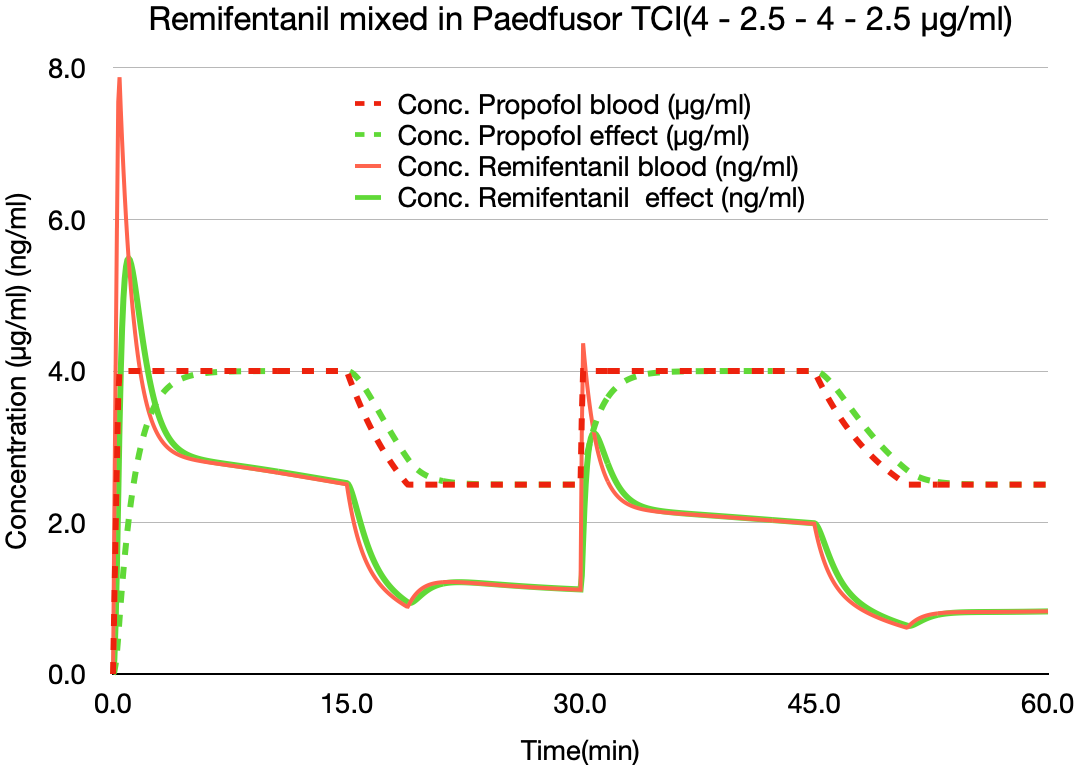
One of the advantages of (Effect)TCI is that a change in target aims to give a time independent proportional change in blood (or effect site) concentration. So although the propofol concentrations in these simulations of alternating the target from 4 to 2.5 µg/ml every 15 minutes with the paedfusor, follow the target setting, this is obviously not the case with the mixed-in remifentanil. What about the Eleveld model?
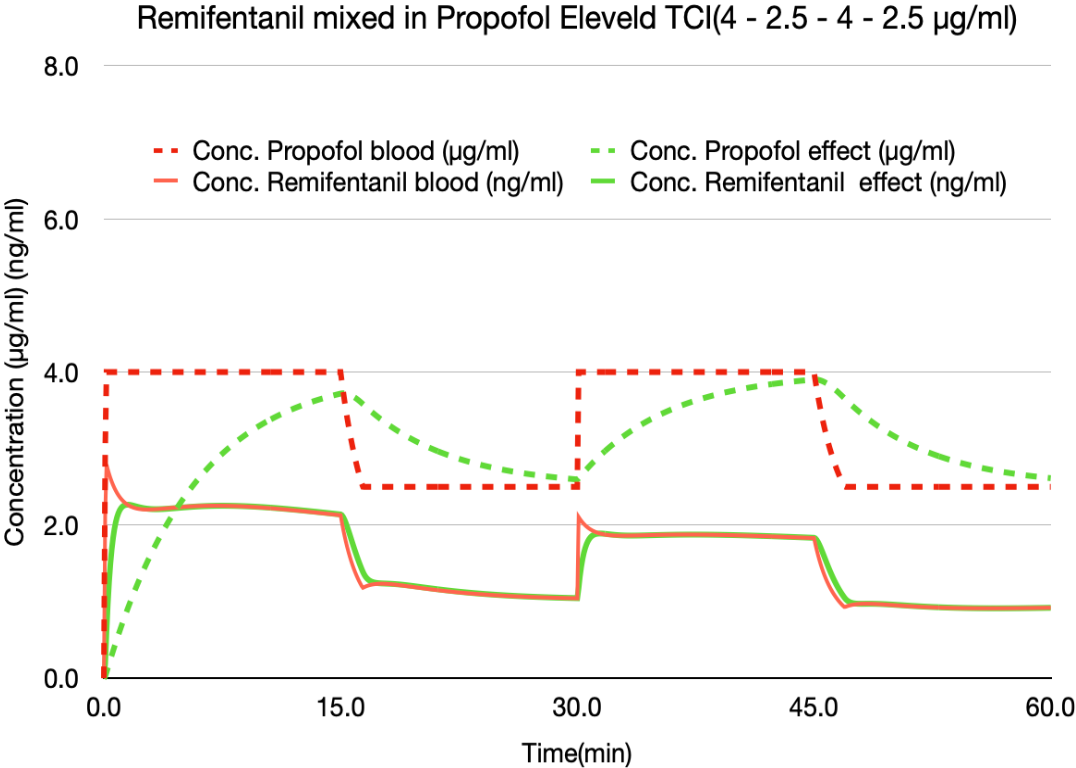
The Eleveld(+opioid) model seems to be a much better base for the mixing with remifentanil. In the previous blog I have explained that this is related to the differences in the size of the central compartment. So solution found? not quite. Look at the slow increase in the effect site concentration of propofol. It will take more than 15 minutes to have a stable effect site concentration. So in practice anaesthesiologist will be tempted to use effect site control. This will achieve an effect site concentration as fast as possible without overshoot for propofol but not for remifentanil:
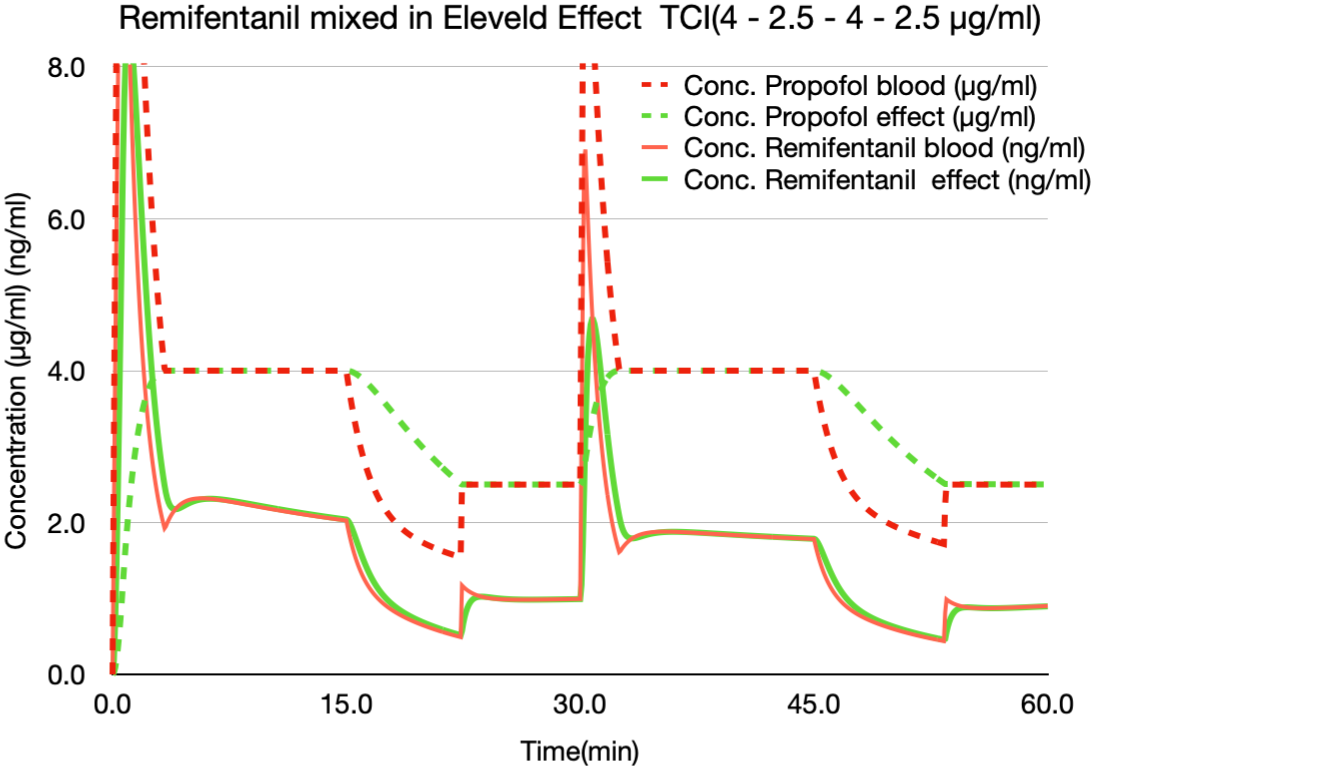
The resulting changes in the remifentanil are even more uncontrolled than with the Paedfusor model. The way a TCI system controls the blood or effect site are the most disturbancing factors in this mixing problem. The TCI device gives a bolus type infusion when increasing the concentration and stops the pump for a varying amount of time when decreasing the concentration. This is all done within the context of the filling state of the underlying 3 compartment model and hence dependent on the moment in anaesthesia the targets are changed. So what about avoiding TCI and using a manual controlled infusion? One of the proposed manual scheme for paediatric TIVA is from McFarlan et all:
https://doi.org/10.1046/j.1460-9592.1999.00364.x
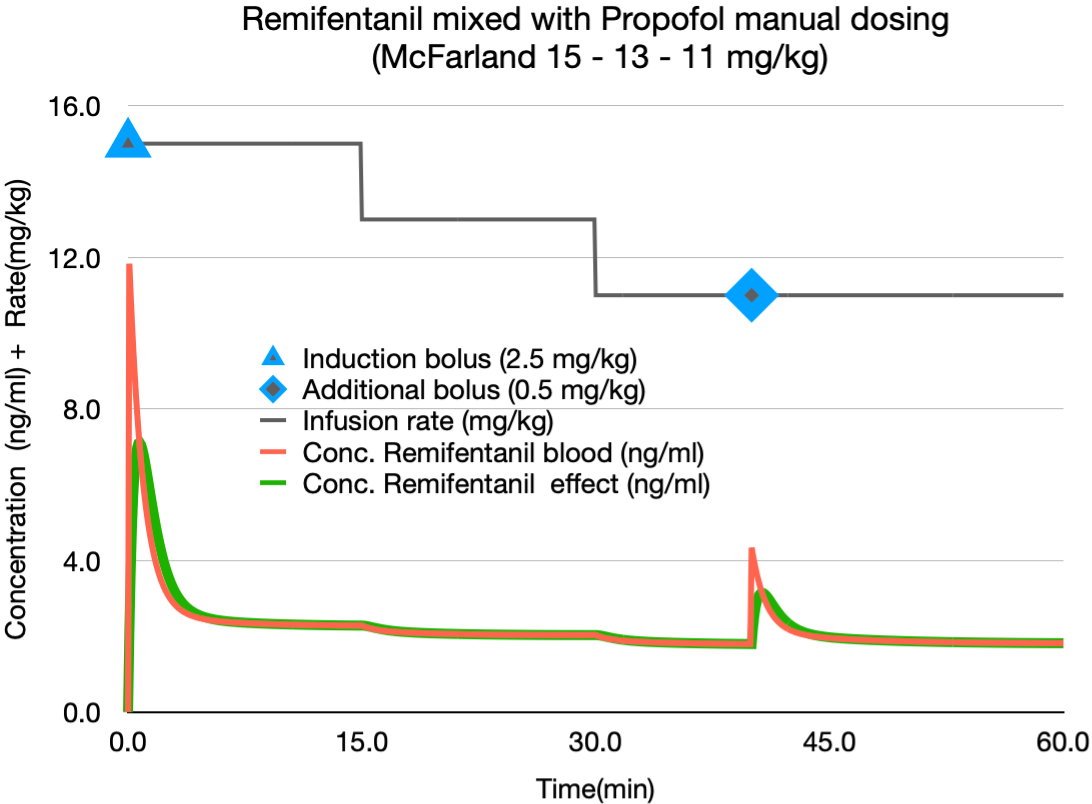
In this simulation there is no effect from stopping and starting the TCI pump. This results in a much more stable remifentanil concentration. Obviously there is an overshoot in the remifentanil at induction because of the bolus propofol. The extra bolus is added to show the effect of a small(0.5 mg/kg) additional bolus. The manual scheme will give a blood propofol concentration of just above 4 µg/ml according to the Eleveld model:
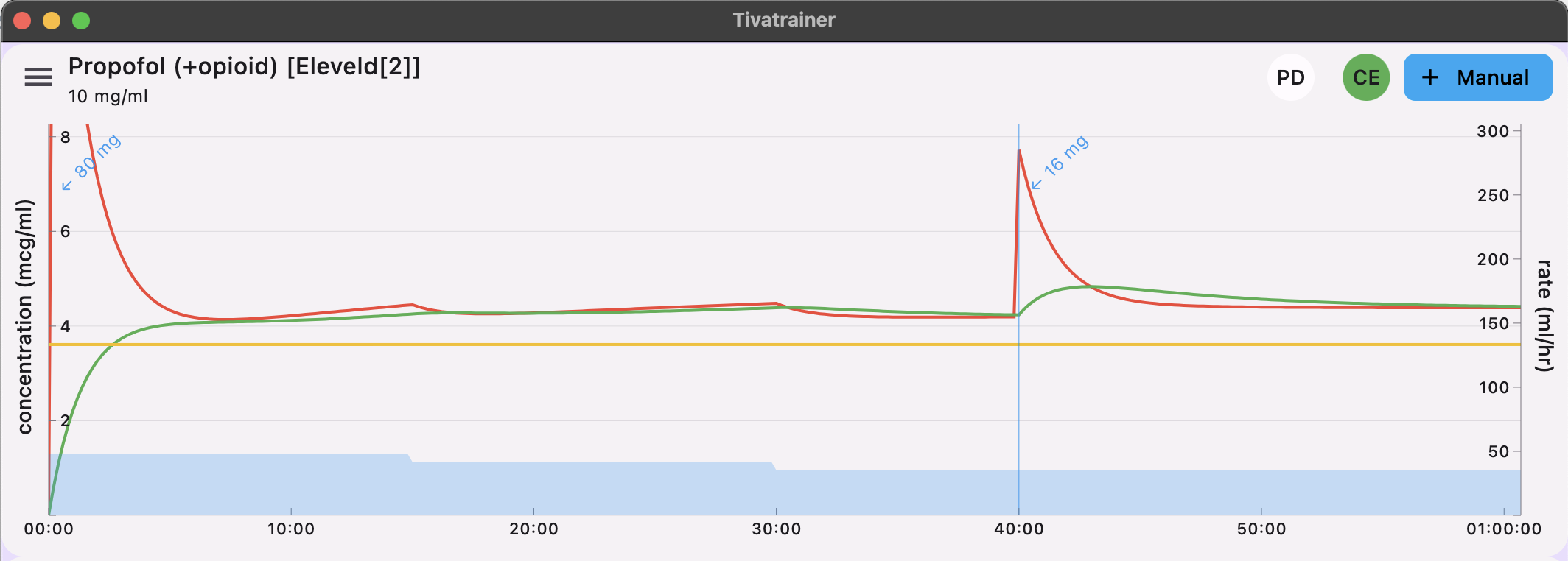
Of course you do not need to give the induction dose with the mixture and also the additional dose can be given with or without Remifentanil, dependent on the clinical situation.
So my final conclusion is: mixing remifentanil with propofol is a bad idea for more than one reason, however if you ever find yourself in a situation with only one infusion pump available and you still need to give TIVA then do not use the pump in TCI mode and certainly not with effect site TCI . Use Tivatrainer with IVAssist (like McFarland did in the publication of the above dosage scheme) to work out a manual scheme that will give you Ce50 with the Eleveld(+opioid) model. In the Eleveld model both pharmacokinetics and pharmacodynamics are adjusted by the anthropometrics of the patient(age, weight,length,gender).
Remember that the Ce50 in the Eleveld model corresponds with a BIS of about 45 which is considered an adequate level of hypnosis in most cases (in other pharmacodynamic models this would correspond with a Ce90 to Ce95).
Prepare your mixture but deliver the induction dose with propofol alone in a separate syringe. This will prevent the overshoot in the remifentanil concentration as seen when using effect TCI. As the remifentanil builds up quickly you could give the induction dose a minute or so later after starting the infusion of the Propofol-Remifentanil mixture thereby using the analgesic effect of remifentanil that is already present. The obtained concentrations of remifentanil are on the very low side ( 1.6-1.4 ng/ml) for general anaesthesia so you may have to ad another analgesic and/or increase the concentration of remifentanil to 0.01 mg/ml for example. Here is a simulation with both remifentanil concentrations.

The inputs for the IVAssist mode can be accessed and changed in the settings window:inputs. For allowing only the infusions to be copy/pasted (see previous blog) the induction bolus has been set to zero first, then the copy/pasting was done (as only the infusions are with the mixture) and then the bolus 2.3 mg/kg was put back in.
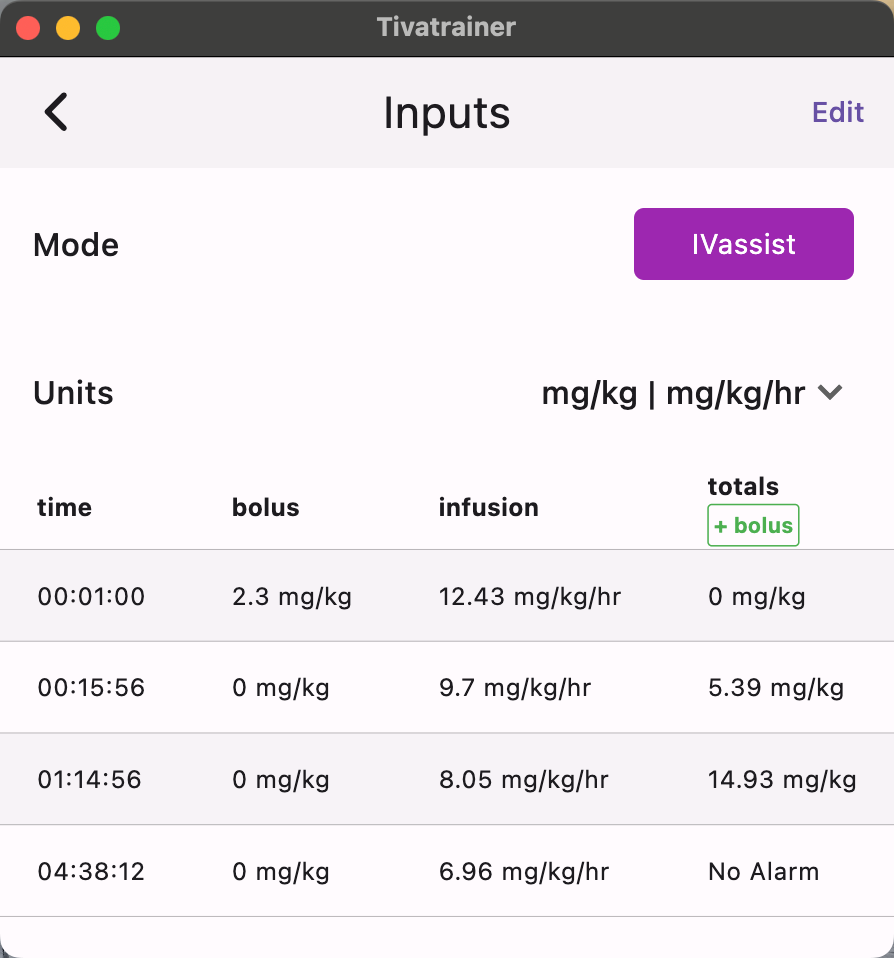
If you want to have a real time info on the plasma and effect site concentration you can used the cursor in the Tivatrainer window (long press) and adjust it to the point were the totals match the volume displayed on your infusion pump.
Please beware:this is not a dosing advice but an educated theoretical approach that can help you in developing your own dosing scheme for a specific clinical scenario where only one infusion pump(in the whole hospital?) is available.
I wonder if the water soluble Remimazolam will resolve the inhomogeneous mixture problem.
One of the advantages of TCI is the fact that it simplifies communication about anaesthesia with TIVA (certainly when we have agreed on the one model principle in the future). But the possible plethora of mixtures and recipes is in my opinion a step backwards by creating a turmoil of anaesthesiologist-dependent TIVA techniques. Being able to control the hypnotic and analgesic part of anaesthesia separately is a great feature of TIVA. It allows a fine-grained control that can be adjusted for the individual patient.
Happy to hear your comments.
PS: on the Euroanaesthesia 2024 meeting in Munich (26 May 2024) Peter Brooks and Mike Irwin will have a pro/con debate on this subject.