The Mixifusor with Tivatrainer: using the Eleveld+opioid model


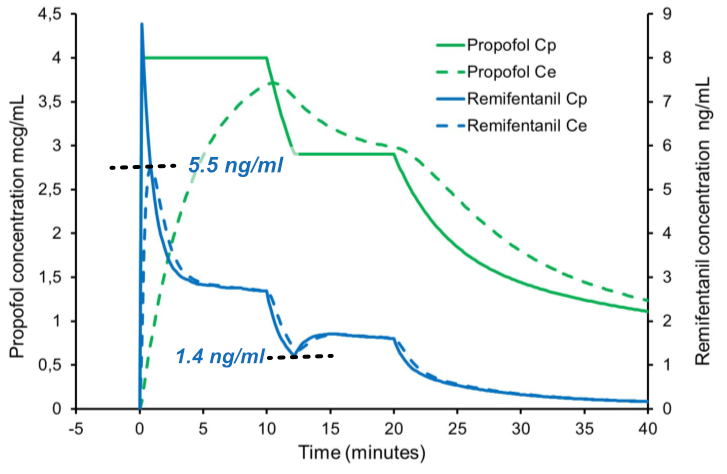
In the preceding blog post, I conducted an analysis of a publication by Absalom et al. focusing on the drawbacks associated with the concurrent administration of propofol and remifentanil, utilising Target Controlled Infusion to regulate propofol levels while making remifentanil dependent on the rate of propofol administration. This 'Mixifusor' method, often employed in pediatric anesthesia, was simulated based on the Paedfusor model for propofol and the Eleveld model for remifentanil, using patient parameters of a 10-year-old male weighing 32 kg and measuring 140 cm. In addition to various disadvantages such as legal implications, increased potential for drug preparation errors, and challenges related to physical mixing, the authors highlighted the instability and unpredictability of remifentanil concentrations due to pharmacokinetic differences between propofol and remifentanil. Figure 2 in the publication illustrates the uncontrolled peak blood and effect site concentrations of remifentanil when the propofol target is raised, and vice versa when the target of propofol is lowered, resulting in a period of low remifentanil concentrations.
To mitigate the initial peak concentration, a staged approach in the first target of propofol is depicted in figure 3 of the publication.
As promised in the prior blog post, I aim to demonstrate the ease of use of Tivatrainer to handle these kind of complex simulations with a step by step guide. The combination of drugs, specifically propofol and remifentanil, in a single syringe controlled by a pharmacokinetic algorithm poses clinical challenges due to the diverse combinations and settings available, including varying dilutions and selections of pharmacokinetic models involved: Paedfusor, Kataria, Eleveld for control of TCI propofol in paediatric cases, and Minto, Eleveld, and different keo's for the connected remifentanil.
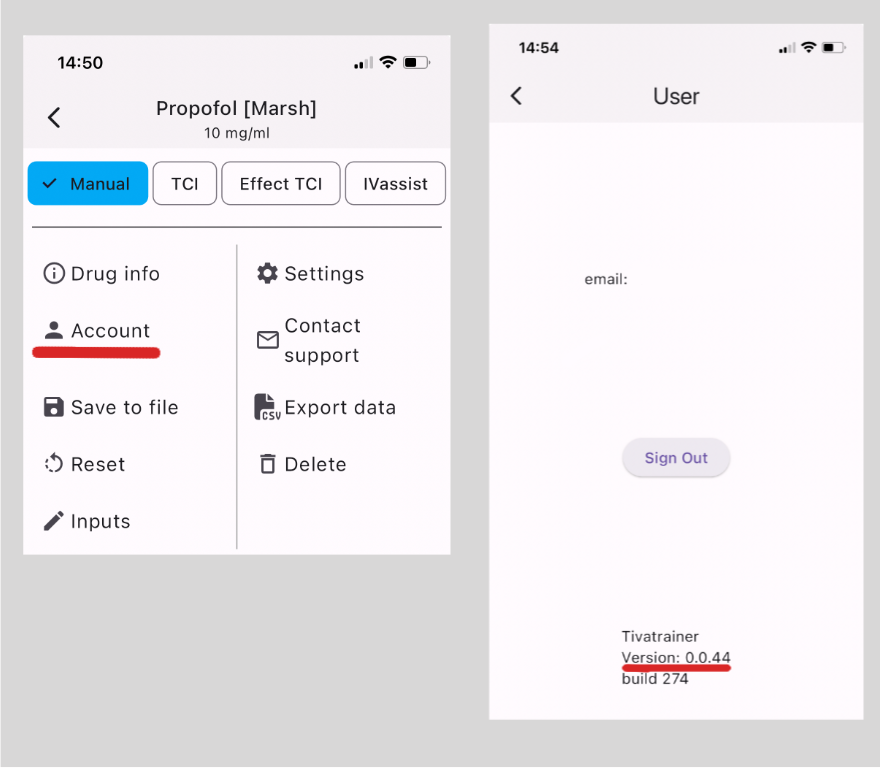
First you need a copy of the Tivatrainer software that is downloadable from www.tivatrainer.com. iOs users also need to download TestFlight for the time being. If you already are using tivatrainer make sure you have version 0.0.44 or higher. You can check your version on your account page in tivatrainer.
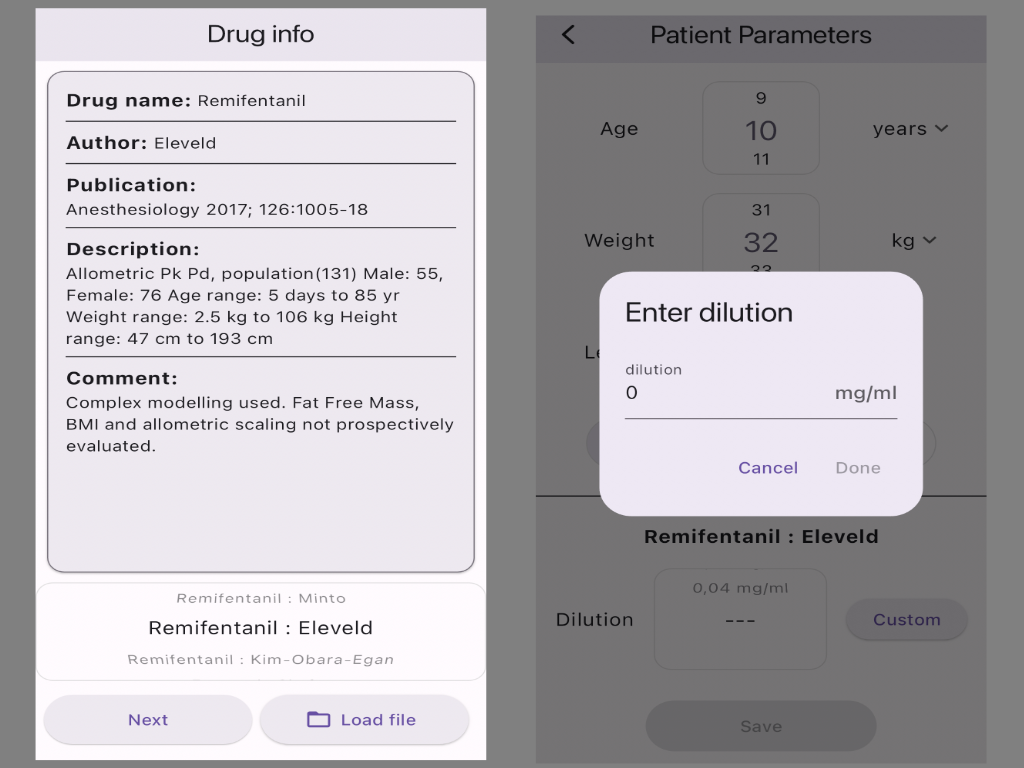
1. Open Tivatrainer and select the Eleveld+opioid model for propofol and press next
2. Enter the patient data as shown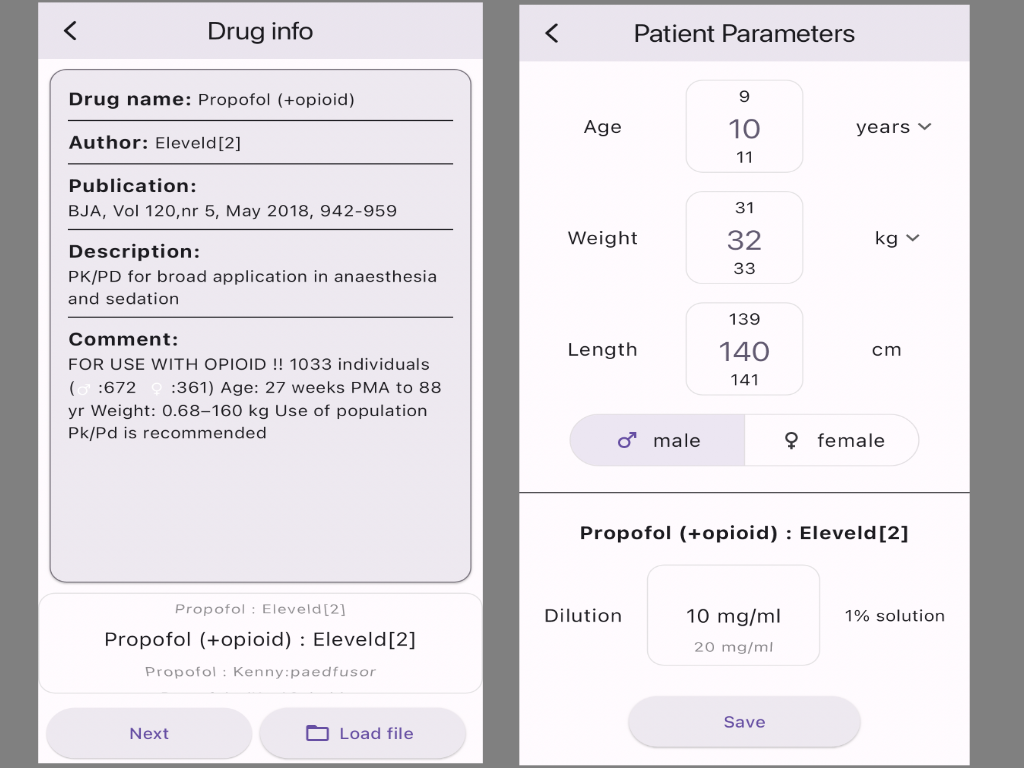
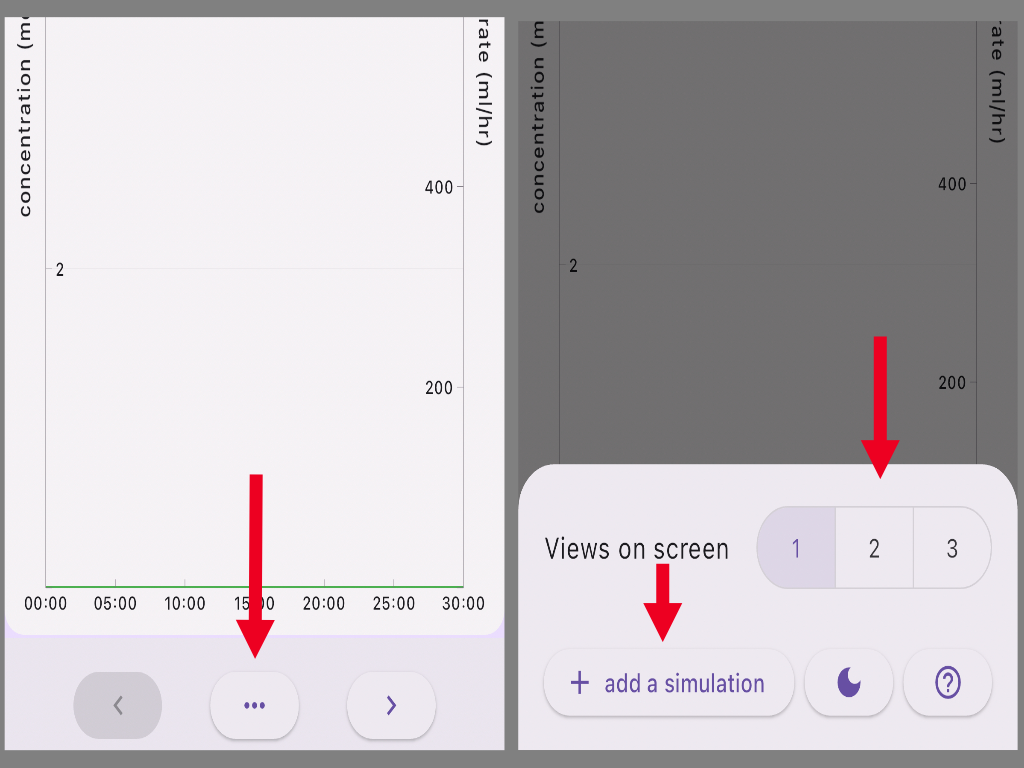
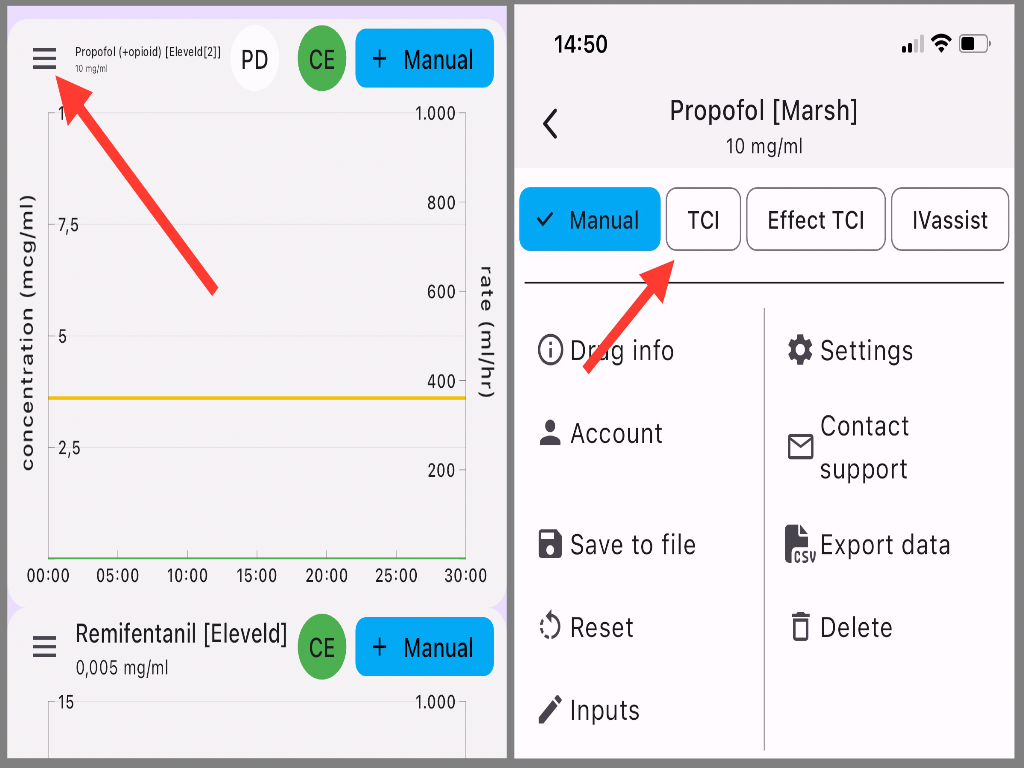
3. Press the 3 dots at the bottom of the screen
4. select 2 views on screen and +add a simulation
5.Select Remifentanil Eleveld and press enter
6.Patient paramaters are maintained, scroll the dilution down until Custom appears and enter the dilution of remifentanil in the propofol syringe: 0.005 mg/ml
7. You now have two simulation windows propofol and remifentanil. Set the mode for propofol to TCI by pressing the harmonica button at the top left of the simulation screen and TCI
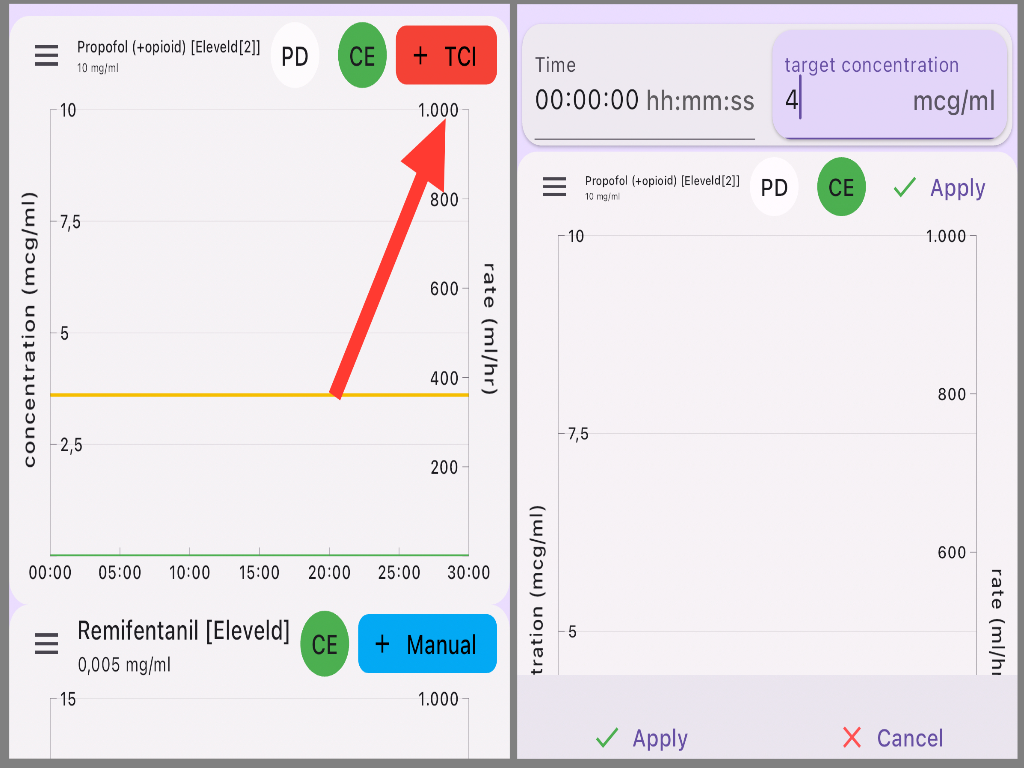
8. Go back to the simulation and press the red +TCI button enter a target of 4mcg/ml at timepoint 00:00:00 and press apply!
9. Go back to the settings screen by pressing the harmonica button at the top left of the simulation screen and press the copy button at the bottom of the screen. Go back to the simulations screen and select the settings screen of the remifentanil simulation and select paste at the bottom.
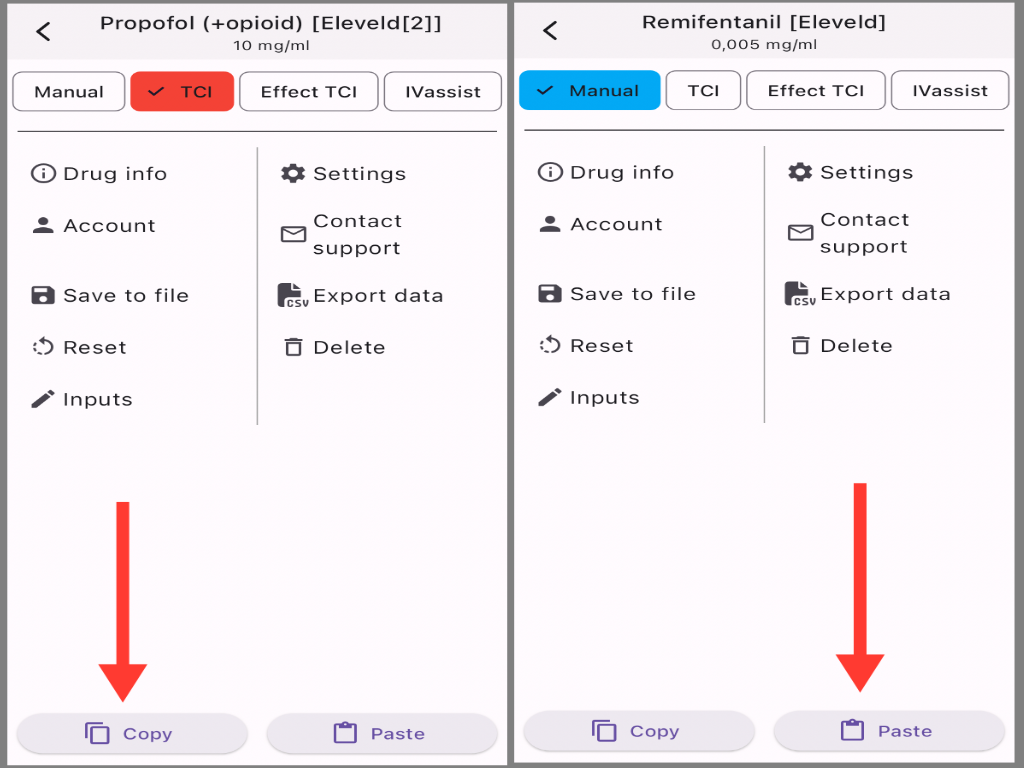
You now have copied the infusion rates from the propofol simulation into the remifentanil simulation
To complete the comparison with the simulations in the publication
10. Go back to the Propofol simulation and press the Red +TCI button. Change the target to 2.9 mcg/ml at 00:10:00 minutes , apply and repeat the copy/paste procedure from step 9
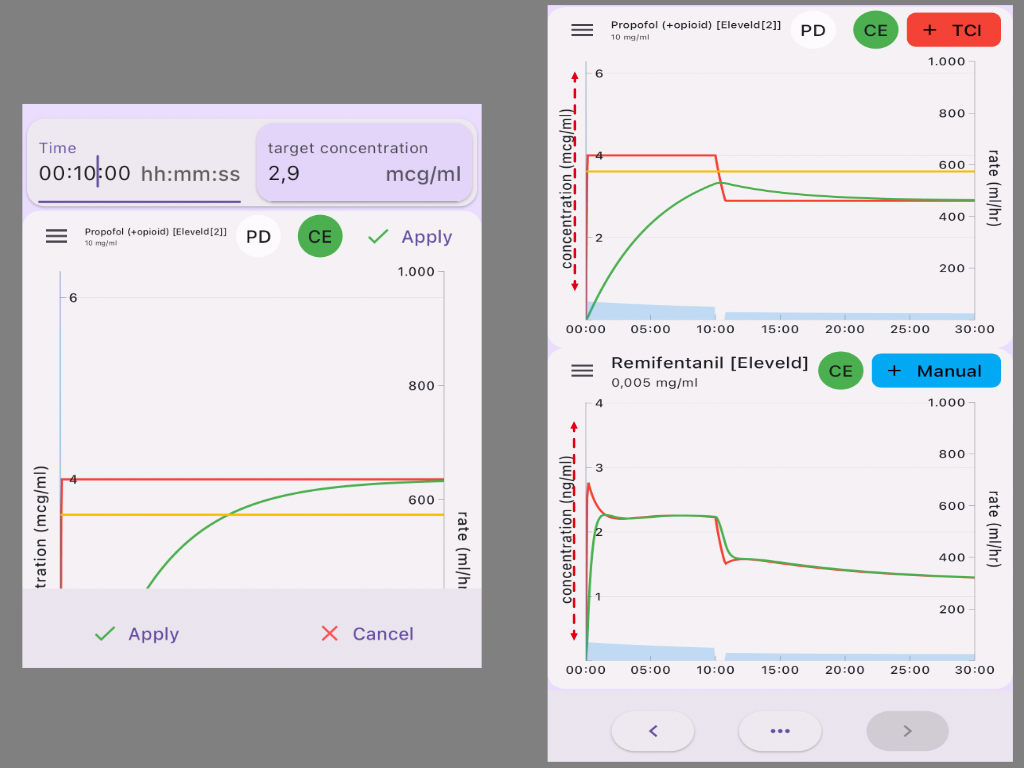
If you followed this guide, the simulation on the right would be on your screen. You can adjust the scaling by dragging on the axis.
Compare this with the figure 2 from the publication of Absalom. Paedfusor with remifentanil overshoots to a Ce of 5.5 ng/ml with a nadir of 1.4 ng/ml with decreasing target. You will notice minimal over and undershoot in the remifentanil blood concentration and none in the effect site concentration when the Eleveld+opioid model is used for TCI propofol.
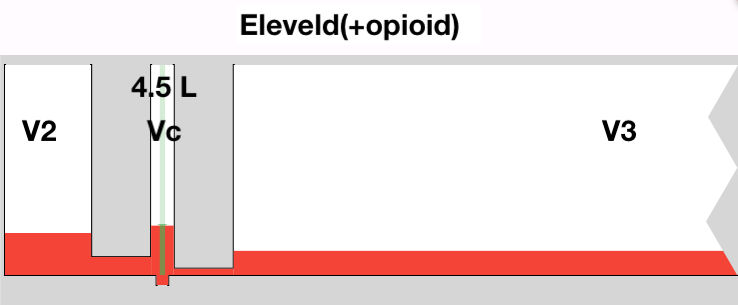
Why? The explanation is mainly the size difference in the central compartment. Select the settings screen for propofol, select drug info, select kinetic parameters. The V1 reads 4.5 L To create a concentration of 4 mcg/ml in V1 you would need a bolus of 4500 ml x 4= 18000 mcg = 18 mg = 1.8 ml
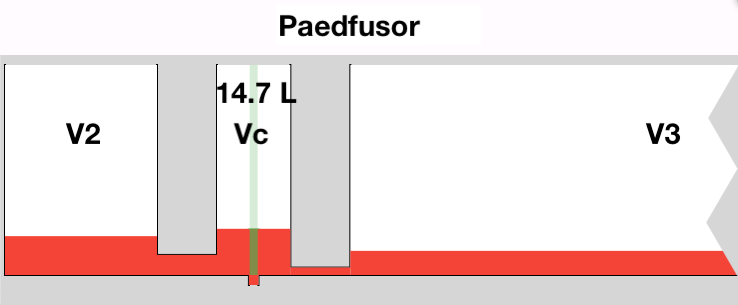
The central volume in the peadfusor for this patients 14.67L which requires a loading volume of 5.8 ml. With the fixed concentration of 0.005 mg/ml remifentanil in the propofol about 3 times more remifentanil is delivered.
When the Propofol target is decreased the pump stops for a certain period to allow the concentration of propofol to decrease by redistribution and elimination. The longer the pump stops the lower the remifentanil concentration will be as the clearance is much faster from remifentanil.
The time the pump stops is dependent on the context sensitive decrement time:the longer the TCI runs the longer the decay time . With Tivatrainer it is easy to setup a scenario with multiple drugs. For example you can start a simulation with the paedfusor set it to TCI, start another simulation with Eleveld(+opioid) for propofol also in TCI mode and then copy paste the simulation between the propofol simulations and thereafter select one of the propofol simulations to the remifentanil. In this YouTube video an advanced example has been worked out for longer simulations.
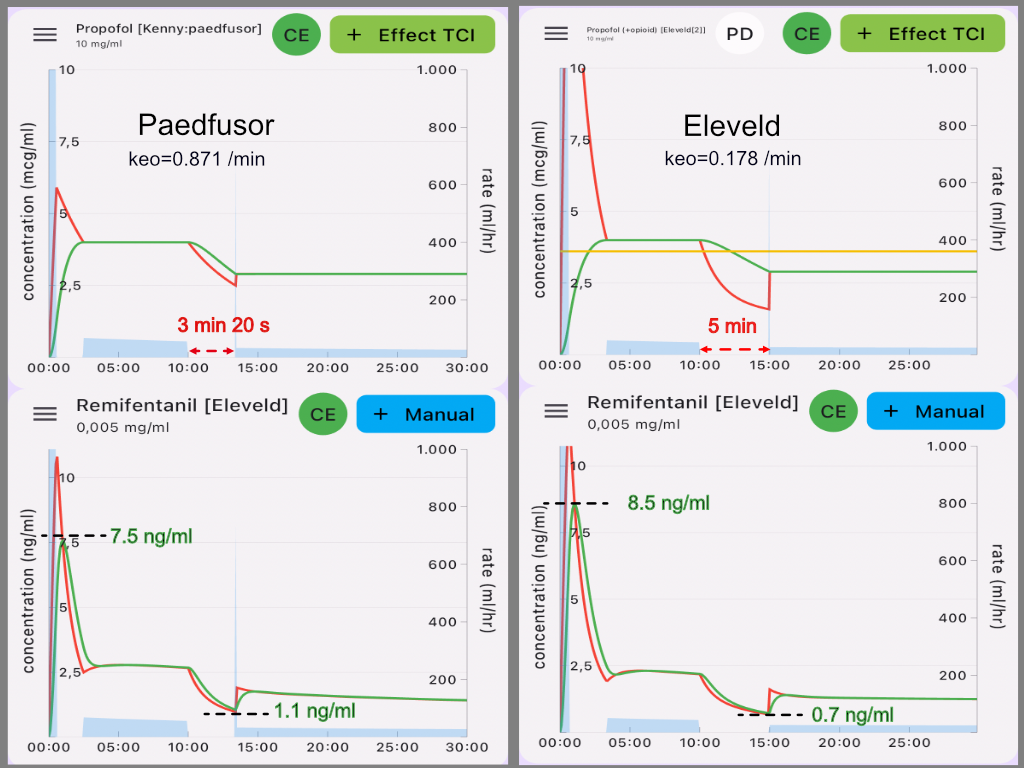
The simulations above are all done with plasma control TCI. I am not aware of commercial TCI pumps that allow effect site control for paediatric patients but considering the implementation-chaos of models and co-parameters it cannot be ruled out that at some point Effect site TCI for paediatric patients may be implemented. Effect site control will highly influence and destabilise the remifentanil concentration when drugs are mixed like with the Mixifusor approach. The instability in the corresponding remifentanil concentrations is even worse than shown in fig 2 of the original publication on the Mixifusor. An important parameter is the blood-brain equilibration constant: keo. A general rule dictates that the smaller the keo(the longer thalfkeo) the bigger the induction dose in ETCI. The advantage of the Eleveld model in plasma control is nullified by the small keo of the model and hence the relative large induction dose for effect site control.
The copy and paste functionality in Tivatrainer is a robust feature, as illustrated previously. It can be particularly useful in comprehending the implications of transitioning from previous models to new global models for TCI. This blog was created with the purpose of serving as a guide for the copy / paste process. In the upcoming blog post, I will outline the conclusions drawn from these simulations regarding the utilisation of diluted remifentanil in a propofol Target Controlled Infusion Device.